
Vitamin D is often treated like a simple add-on to a daily routine, but it does not always act like a harmless extra. Because it influences calcium balance, absorption, and metabolism, it can interact with several widely used medications in ways that matter for safety, monitoring, or timing.
Some combinations mainly reduce how well vitamin D is absorbed. Others can raise calcium levels or intensify side effects already linked to a prescription drug. The key issue is not that these pairings are always unsafe, but that they may need closer supervision.
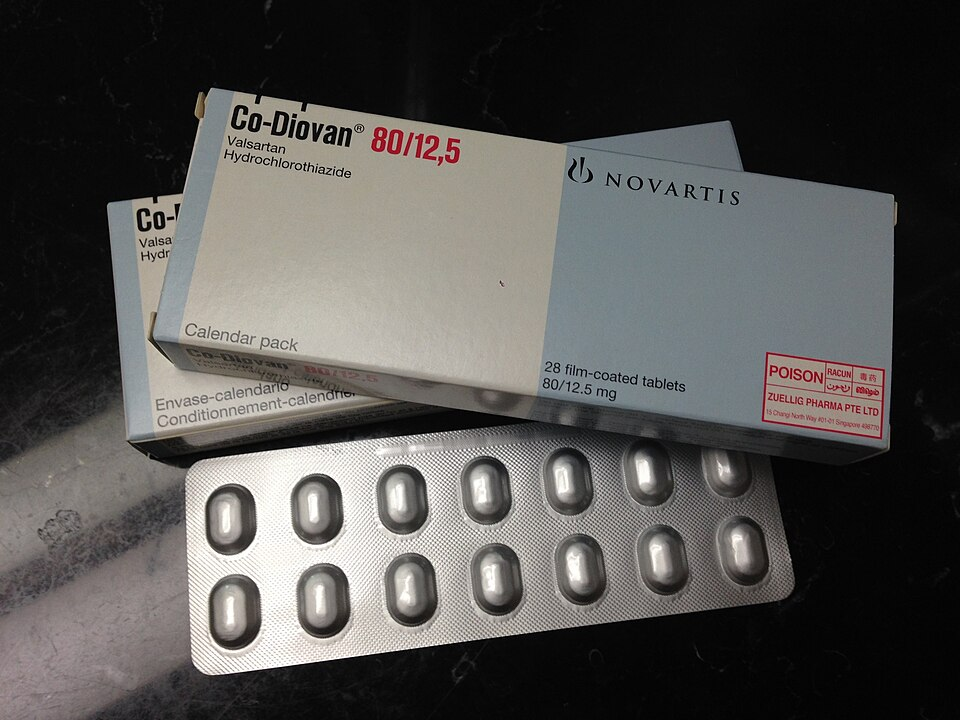
1. Hydrochlorothiazide
Hydrochlorothiazide, a thiazide diuretic used for blood pressure, can raise calcium levels by reducing how much calcium the kidneys excrete. Vitamin D increases calcium absorption from the gut, so the overlap can push calcium higher than expected in some people.
In a study of Black adults taking hydrochlorothiazide, vitamin D3 up to 4000 IU daily was linked to a rise in serum calcium, although clinically significant hypercalcemia was uncommon. That still makes the combination one that may call for lab monitoring, especially in older adults or people with kidney issues.

2. Orlistat
Orlistat reduces fat absorption, which can also reduce absorption of fat-soluble vitamins, including vitamin D. That means a person may be taking vitamin D consistently but still not absorb it well enough to maintain healthy blood levels. Drug-interaction guidance notes that orlistat can interfere with the absorption of cholecalciferol. Timing matters here, and clinicians often separate the doses to limit the problem.

3. Digoxin
Digoxin already has a narrow therapeutic window, which is why anything that shifts calcium balance deserves attention. Vitamin D can raise calcium absorption, and excess calcium may increase the risk of rhythm-related complications in people taking digoxin.
This interaction becomes especially important when vitamin D supplements are taken alongside calcium products. The concern is not routine vitamin D use alone in every patient, but the possibility of compounding calcium-related effects that can make digoxin harder to manage safely.
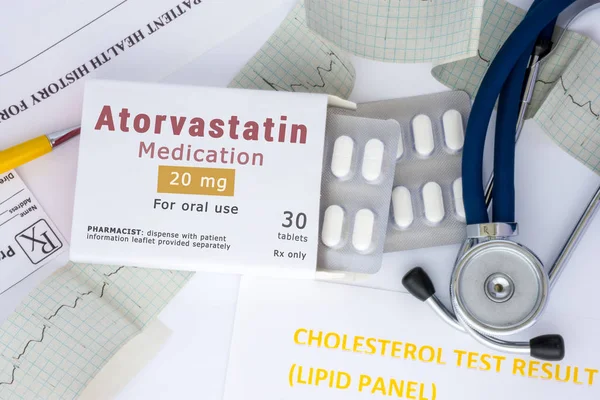
4. Atorvastatin
Atorvastatin does not appear to deplete vitamin D in a predictable way. In fact, some studies suggest the opposite: vitamin D levels may remain stable or rise modestly in some statin users. That does not make the pairing a problem in the usual sense, but it does make it a medication relationship worth understanding.
A review of statins and vitamin D found that the overall effect is often neutral or mildly beneficial, rather than harmful. The main practical issue is that muscle pain can overlap between low vitamin D status and statin-associated symptoms, which can complicate assessment.

5. Rosuvastatin
Rosuvastatin stands out because some studies reported larger increases in vitamin D levels after treatment began. The evidence has been debated, but it has kept rosuvastatin in the conversation about vitamin D interactions.
Research cited in the review described an increase in 25-hydroxyvitamin D from about 14 ng/mL to 36 ng/mL over 8 weeks in one observational study. Later analyses questioned how much of that change reflected the drug itself versus outside factors such as seasonal sun exposure.

6. Simvastatin
Simvastatin shares some metabolic pathways with vitamin D, including CYP3A4-related processing. Because of that, it has been studied for possible effects on vitamin D breakdown and blood levels. The evidence is mixed. Some small studies reported increases in vitamin D markers, while others found no meaningful change. The more useful takeaway is that vitamin D should not automatically be blamed for a problem simply because simvastatin is on the medication list, and simvastatin should not automatically be assumed to cause deficiency either.

7. Lovastatin
Lovastatin has also been linked in small studies to higher vitamin D levels during treatment. That does not establish a clinically important benefit for everyone, but it shows that drug-nutrient interactions can move in either direction.
This matters because patients sometimes assume every medication only lowers nutrient levels. With lovastatin, the available data suggest the relationship is more complex, and any decision about supplementation still depends on measured vitamin D status rather than assumption.
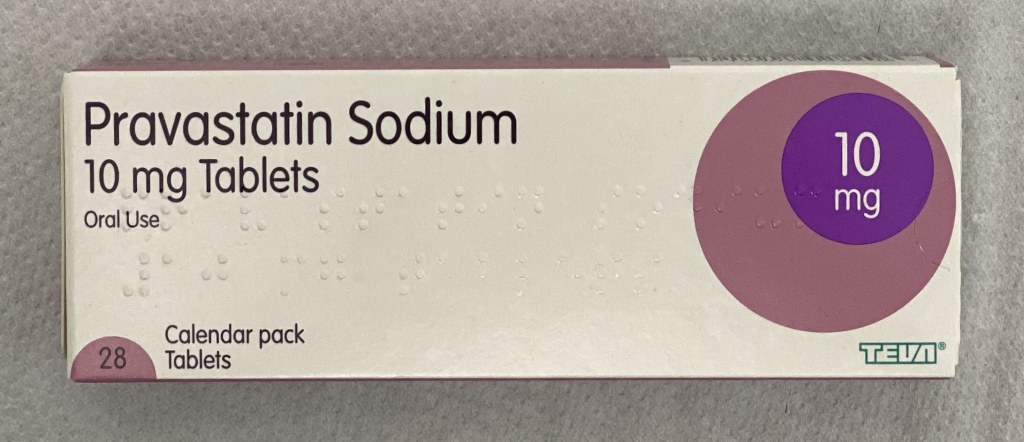
8. Pravastatin
Pravastatin is often discussed as a contrast to some other statins because trials have generally shown little or no effect on vitamin D levels. In other words, this is a pairing where the “interaction” is mostly notable for being minimal. That is still useful clinically. It helps show that statins are not interchangeable in how they relate to vitamin D metabolism, and it reinforces the need to look at the specific drug rather than the whole class as one category.

9. Fluvastatin
Fluvastatin has likewise shown little change in vitamin D levels in comparative research. In the STATIN-D trial discussed in the review, fluvastatin did not produce the same rise in vitamin D that was reported with rosuvastatin. That difference highlights an important point: when vitamin D levels shift during treatment, the change may reflect the individual medication, the person’s baseline vitamin D status, or outside factors such as diet and sun exposure.
The biggest theme across these drug pairings is that vitamin D interactions are not all alike. Some combinations, such as hydrochlorothiazide and digoxin, raise concern because of calcium-related effects. Others, like orlistat, can reduce absorption. Statins are different again, since current evidence does not show that they routinely cause vitamin D deficiency.
For people taking vitamin D alongside prescription medicines, the safest approach is usually simple: review the full medication list, check whether calcium balance or absorption is affected, and use blood testing when symptoms or risk factors make it necessary. That turns vitamin D from a guess into something that can be managed with more precision.

